Narrative
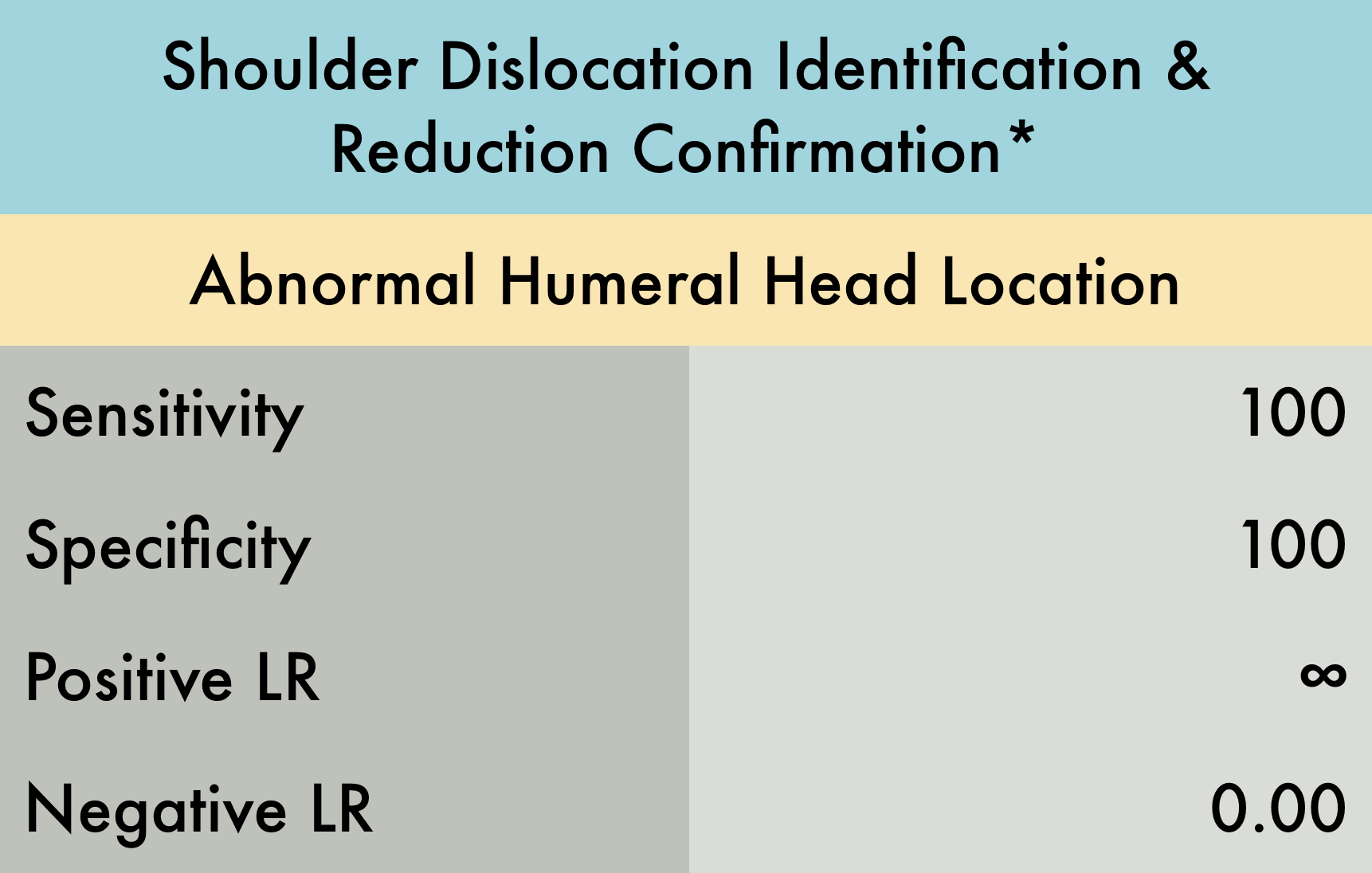
This was a prospective observational study (n= 73) evaluating the diagnostic accuracy of ultrasound for both identification of shoulder dislocation and confirmation of successful reduction. Patients with suspected shoulder dislocation were enrolled, with 69/73 having dislocation confirmed by shoulder radiographs. Patients with multi trauma or decreased level of consciousness were excluded. Both the anterior and lateral approach were used to evaluate for dislocation. Examinations were performed by either an experienced ultrasound trained emergency physician or a senior emergency medicine resident. An ultrasound exam was performed prior to initial shoulder radiographs and after reduction attempt. Ultrasound was found to be 100% accurate with respect to both shoulder dislocation identification and reduction confirmation. *This is a limited study as the sample size is relatively small and this ultrasound examination is dependent on operator experience therefore these results should be interpreted with caution.
Caveats
Note: accuracy of ultrasound is operator-dependent. Reported LRs may not be reproducible by an inexperienced sonographer.
Published in collaboration with The POCUS AtlasAuthor
Mike Macias, MD
Published/Updated
September 13, 2018
What are Likelihood Ratios?
LR, pretest probability and posttest (or posterior) probability are daunting terms that describe simple concepts that we all intuitively understand.
Let's start with pretest probability: that's just a fancy term for my initial impression, before we perform whatever test it is that we're going to use.
For example, a patient with prior stents comes in sweating and clutching his chest in agony, I have a pretty high suspicion that he's having an MI – let's say, 60%. That is my pretest probability.
He immediately gets an ECG (known here as the "test") showing an obvious STEMI.
Now, I know there are some STEMI mimics, so I'm not quite 100%, but based on my experience I'm 99.5% sure that he's having an MI right now. This is my posttest probability - the new impression I have that the patient has the disease after we did our test.
And likelihood ration? That's just the name for the statistical tool that converted the pretest probability to the posttest probability - it's just a mathematical description of the strength of that test.
Using an online calculator, that means the LR+ that got me from 60% to 99.5% is 145, which is about as high an LR you can get (and the actual LR for an emergency physician who thinks an ECG shows an obvious STEMI).
(Thank you to Seth Trueger, MD for this explanation!)
