Narrative
Penetrating extremity trauma (PET) is a common cause of arterial injury in the United States. PET can result in amputation, wound infection, venous thromboembolism, need for surgical interventions such as fasciotomy, and death. The diagnosis of arterial injury in patients with PET has been the subject of debate with differing recommendations by professional society and major trauma guidelines (Table 1).,
The systematic review discussed here assesses the accuracy of the ankle–brachial index (ABI) in the diagnosis of arterial injury in patients with PET. The systematic review identified five prospective studies of 1,040 adult patients with upper or lower PET who underwent ABI. The prevalence of arterial injury was 14.3%. Due to considerable heterogeneity (I2 >75%), the authors chose not to calculate a pooled positive likelihood ratio (LR+) for ABI. The pooled negative likelihood ratio (LR–) for ABI was 0.59. Although this review concluded that ABI cannot independently exclude arterial injury, the systematic review suggested that such injuries can be excluded in patients with no hard or soft signs and a normal ABI (≥0.9).
Caveats
There are some limitations of the systematic review and metaanalysis. While all studies were prospective and the majority at low risk of bias, a considerable degree of heterogeneity existed among studies with regard to physical examination findings for arterial injury. The authors attributed this heterogeneity to the varying definition of hard and soft signs of arterial injury used across the included trials that originated from discrepancies in major trauma guidelines (Table 1).
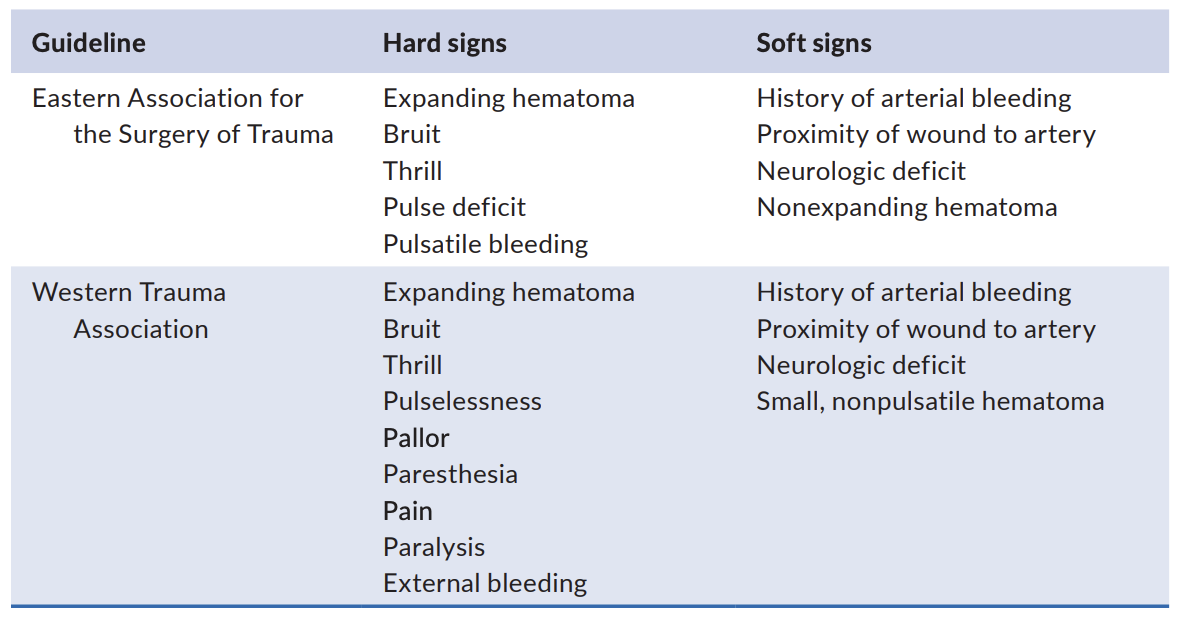
Table 1. Definition of hard and soft signs in trauma guidelines
Another limitation of the analysis is that not all patients received the reference standard diagnostic study. In almost all of the included trials, low-risk patients were observed for 24 h and did not undergo any of the predetermined reference tests: CT angiography, catheter angiography, or surgical exploration. The probability of clinically significant arterial injury (requiring intervention) in this population is likely to be low but cannot be accurately reported. A significant portion of these “low-risk” patients were then discharged and were lost to follow-up. This, therefore, creates risk of partial and differential verification bias.
Due to considerable heterogeneity, the systematic review did not report the posttest probability of arterial injury in patients with no hard signs of vascular injury. However, in patients with no hard or soft signs of vascular injury, a systematic review concluded that arterial injury can be ruled out if ABI is normal (≥0.9). This conclusion was drawn from two trials that included a group of PET patients without any hard or soft signs of arterial injury that underwent ABI testing. The review reports a pooled LR– of 0.01 for negative ABI in absence of soft or hard signs of vascular injury. The authors used the weighted prevalence of arterial injury in this subgroup of patients (16.3%) as an estimate of the pre-test probability and applied LR– of 0.01, arriving at a posttest arterial injury probability of 0% (95% CI = 0% to 1%). Based on this calculation, they suggested that this subset of patients may not need further testing. One limitation of this recommendation is its applicability in patients with PETs when the trajectory of injury is in proximity to a major artery. In contrast to the guidelines,
, these two studies did not classify trajectory of injury in proximity to a major artery as a soft sign. In patients with such injuries, therefore, the review recommends that clinicians use their clinical judgment to decide whether to discharge, observe, or obtain further testing.
In summary, the existing evidence suggests that a normal ABI in the absence of soft or hard signs may rule out the presence of arterial injury in patients suffering from penetrating extremity injury. The data are insufficient to draw any conclusions about the use of ABI in any other penetrating extremity injury scenario.
The original manuscript was published in
Academic Emergency Medicine as part of the partnership between TheNNT.com and AEM.
Author
Roshanak Benabbas, MD; Ian S. deSouza, MD
Supervising Editor: Kabir Yadav, MD
Published/Updated
April 30, 2021
What are Likelihood Ratios?
LR, pretest probability and posttest (or posterior) probability are daunting terms that describe simple concepts that we all intuitively understand.
Let's start with pretest probability: that's just a fancy term for my initial impression, before we perform whatever test it is that we're going to use.
For example, a patient with prior stents comes in sweating and clutching his chest in agony, I have a pretty high suspicion that he's having an MI – let's say, 60%. That is my pretest probability.
He immediately gets an ECG (known here as the "test") showing an obvious STEMI.
Now, I know there are some STEMI mimics, so I'm not quite 100%, but based on my experience I'm 99.5% sure that he's having an MI right now. This is my posttest probability - the new impression I have that the patient has the disease after we did our test.
And likelihood ration? That's just the name for the statistical tool that converted the pretest probability to the posttest probability - it's just a mathematical description of the strength of that test.
Using an online calculator, that means the LR+ that got me from 60% to 99.5% is 145, which is about as high an LR you can get (and the actual LR for an emergency physician who thinks an ECG shows an obvious STEMI).
(Thank you to Seth Trueger, MD for this explanation!)
