
Corticosteroids for Treating Pneumonia

Benefits in NNT
17
NNT of 17 for preventing death in patients with severe pneumonia (pneumonia severity index score >4 or equivalent)
33
NNT of 33 for reducing risk of new respiratory failure
5
NNT of 5 for reducing risk of shock
Shorter length of hospital stay by average of 3 days
Shorter length of intensive care unit stay by average of 2 days

Harms in NNT
11
NNH of 11 for elevated blood sugar (hyperglycemia)
View As:
Source
Stern A, Skalsky K, Avni T, Carrara E, Leibovici L, Paul M. Corticosteroids for pneumonia. Cochrane Database Syst Rev 2017;(12):CD007720.Study Population: 2,264 adults and children admitted to the hospital with community-acquired pneumonia from 17 trials
Efficacy Endpoints
All-cause 30-day mortality, risk of new respiratory failure, risk of shock, length of hospital and intensive care unit stayHarm Endpoints
Hyperglycemia, secondary infections, neuropsychiatric complications, and gastrointestinal bleedingNarrative
Pneumonia remains a major cause of morbidity and mortality in the United States.1 There is both theoretical and laboratory evidence that corticosteroids may have beneficial effects in pneumonia through local pulmonary and systemic effects.2, 3The data for this evidence-based summary are derived from a Cochrane meta-analysis by Stern et al.,4 which included 17 trials with 2,264 adult and children admitted to the hospital with community-acquired pneumonia (CAP). We will also discuss another systematic review by Briel et al.5 that included 1,500 patients from six randomized controlled trials.
The Cochrane systematic review4 included adults and children hospitalized with CAP with or without health care-associated pneumonia. Patients were randomized to receive corticosteroids (any dose and any duration) plus usual care or placebo plus usual care. The most common dose given was the equivalent of 40 to 50 mg of prednisone daily for 5 to 10 days. This meta-analysis4 showed that corticosteroids decreased 30-day all-cause mortality in adults with severe pneumonia defined as pneumonia severity index score >4 or equivalent with a number needed to treat (NNT) of 17 (Table 1). In the entire cohort of patients (severe and nonsevere pneumonia), administration of corticosteroids was associated with a lower risk of new respiratory failure (defined as requiring noninvasive or invasive mechanical ventilation) and a reduced risk of shock with NNT of 33 and five, respectively (Table 1). Length of hospital and intensive care unit stays were also shortened for all adult patients (mean difference = –3 days; 95% confidence interval [CI] = –5 to –0.9; mean difference = –2 days; 95% CI = –2.96 to –0.81, respectively).4
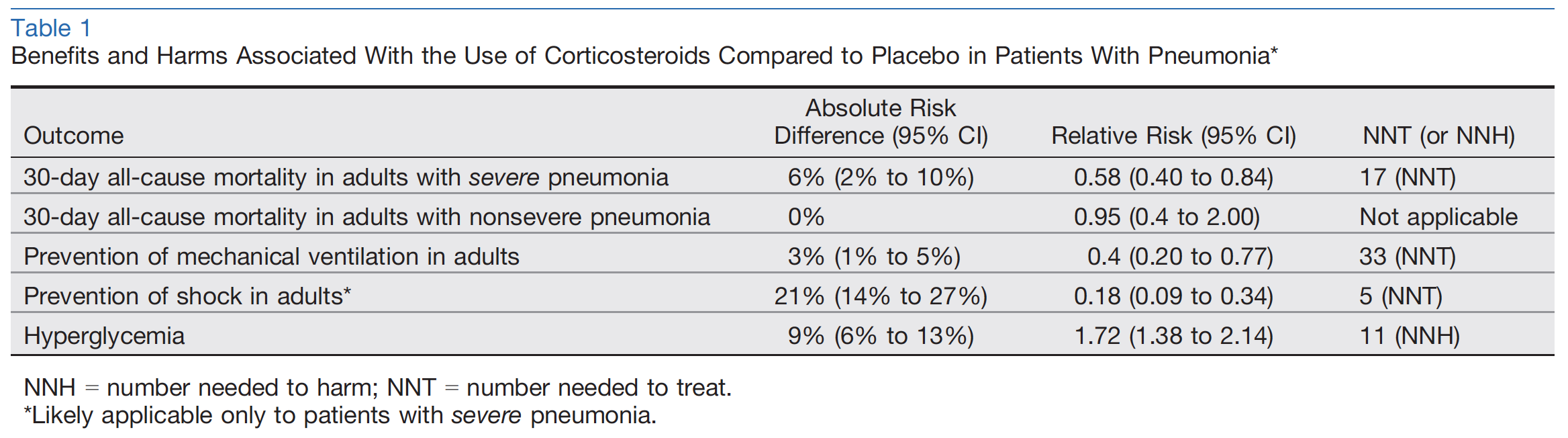
The only adverse event associated with the use of corticosteroids was hyperglycemia with number needed to harm (NNH) of 11 (Table 1).4 However, hyperglycemia was not clearly or consistently defined. The risks of secondary infections, neuropsychiatric complications, gastrointestinal bleeding, and other adverse events were not significantly different between the groups.4
Briel et al.5 conducted a patient-level analysis (Cochrane was a trial-level analysis) based on data from six trials and found that corticosteroids had no clear mortality benefit neither in all cases of pneumonia (odds ratio [OR] = 0.75, 95% CI = 0.46 to 1.21) nor in severe pneumonia (OR = 0.70, 95% CI = 0.44 to 1.13). This meta-analysis confirmed shorter length of hospital stay for patients who received corticosteroids by >1 day but the rate of 30-day pneumonia-related rehospitalization was higher (5% vs. 3%; OR = 1.85, 95% CI = 1.03 to 3.32; NNH = 45). Pneumonia-related rehospitalization was defined as recurrent pneumonia, other infection, pleuritic pain, adverse cardiovascular event, or diarrhea. Corticosteroid treatment was associated with higher incidence of hyperglycemia.5
Caveats
The main limitation of the evidence for mortality benefit of corticosteroids in severe pneumonia according to the Cochrane meta-analysis4 is the possibility of bias, as the only positive effect on mortality was found in trials with unclear risk of bias.4 For this reason, the Cochrane authors downgraded the level of evidence from high to moderate.There is also a notable discrepancy between the two meta-analyses for this outcome. One reason for this discrepancy is that Briel et al.5 only included six trials in the meta-analysis while Cochrane included 17 trials.4 Briel et al. excluded several trials because patientlevel data were not available.5 These six trials were all included in the Cochrane analysis. Therefore, the analysis by Briel et al.5 was performed on only a subgroup of patients included in the Cochrane data set.4 Given the similarity of the effect estimate for mortality rate in severe pneumonia between both meta-analyses as well as a wider 95% CI in the analysis by Briel et al. compared to that of Cochrane (OR = 0.70, 95% CI = 0.44 to 1.13; vs. OR = 0.58, 95% CI = 0.40 to 0.84), it is likely that the exclusion of the trials without patient-level data reduced the statistical power in the analysis by Briel et al.4, 5
For the outcome of rehospitalization in the meta-analysis of Briel et al., 5% of patients were rehospitalized in the corticosteroid group as opposed to 2.7% in the placebo group (total N = 1,368, full distribution of patients not available due to lack of data).5 On the surface this outcome appears appropriately powered but this is a composite outcome. Patients were rehospitalized for “other infection, pleuritic pain, cardiovascular disease event, diarrhea.”5 Therefore, we feel that the data supporting this negative outcome should be interpreted with caution and it is not specifically powered to measure rehospitalizations directly due to steroid administration.
For the outcome of reducing risk of shock, while the Cochrane review found that there was significant benefit in the steroid arm,4 this effect may be overstated. The pooled risk of development of shock in the control group of the meta-analysis was approximately 24% among 500 patients.4 This rate is significantly higher than the reported rate of patients with CAP requiring vasopressors in the literature (approximately 5%).6 However, three of four of trials included in this outcome analysis were conducted on patients with severe pneumonia, which carry a higher baseline risk of development of shock. Therefore, we suggest that the NNT of 5 should be considered as only applying to patients with severe pneumonia and not necessarily to all patients.
The patient-level analysis approach employed by Briel et al.,5 which usually is used to reduce heterogeneity, offers little advantage over the Cochrane analysis as the heterogeneity of this meta-analysis was already low (I² = 12%, fixed-effect model).4 In our opinion, because of lower risk of type II error and low heterogeneity, the Cochrane review offers a more robust and accurate data set and thus more reliable findings for mortality benefit of corticosteroids in severe pneumonia.4
Children were also included in the Cochrane review4 but they were excluded from most outcome analyses because of paucity of data. Although the Cochrane review rated the quality of evidence for children as high, there were only four studies that enrolled children.4 Additionally, there were no reported deaths in these four trials. Therefore, the findings of this meta-analysis could not be generalized to the pediatric population.
Lastly, patients with pneumonia and a history of chronic obstructive pulmonary disease (COPD) may benefit more from corticosteroids. The Cochrane review did not perform a subgroup analysis to examine the effect of COPD on the results (three of 17 trials excluded patients with COPD). But they performed a meta-regression analysis that did not show an association between the percentage of COPD patients in the trials and corticosteroid mortality benefit.4
Clinical Implications: While the evidence for the mortality benefit of corticosteroids for pneumonia is of moderate quality, there are other patient-centered benefits including shortened hospital stay, prevention of shock, and lower risk of respiratory failure. The combination of improvement in patient-centered outcomes, lower medical costs and resource utilization, and relative safety is desirable not only for patients, but for institutions as well. Therefore, we assign a color recommendation of green (benefits > harms) to this treatment. In summary, the existing evidence supports the use of corticosteroids in patients hospitalized with pneumonia. This recommendation is based on a probable mortality benefit and lower risk of shock in patients with severe pneumonia as well as shorter length of hospital stay and respiratory failure in all patients. Low costs and low risk of adverse events augment these clinical benefits.
The original manuscript was published in Academic Emergency Medicine as part of the partnership between TheNNT.com and AEM.
Author
Peter Tepler, MD; Shahriar Zehtabchi, MDSupervising Editors: Gary Green, MD; James McCormack, MD
See TheNNT.com's previous review of this topic: Corticosteroids for Community-Acquired Pneumonia, June 1, 2016
Published/Updated
March 29, 2019References:
